 MAKESPACE - Start Here
MAKESPACE - Start HereLoading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Loading...
Step-by-step health equity recommendations for COVID-19 communication
This toolkit offers detailed, step-by-step guidance to help health communicators, content developers, educators, and health promotion leaders put health equity recommendations into COVID-19 communication action. The toolkit is a collection of information we at U.S. Digital Response have learned and trends analyzed through evidence-based research such as:
Working with multiple local and state government agencies, including communication specialists and content managers,
Creating content and user experience (UX) recommendations across devices and browsers to impact vaccination information-seeking behavior, and
Our collective decades of experience in health equity, communication, and literacy directly educating and reaching communities.
This is a living document. We will continuously update it as we learn more from government and public health officials, communication teams, and health equity task forces.
If you would like more information or pro-bono support from our teams of technologists at USDR, please reach out. We will get back to you within hours.
This toolkit is for government communications and media development teams, trusted messenger centers, and community-based organizations that are responsible for designing, developing, and evaluating resident-facing COVID-19 digital tools with a health equity lens. These tools include but are not limited to websites, mobile apps, and digital print media with the goal of helping residents find COVID-19 vaccination and testing information easily and seamlessly.
Background: Top communication needs that USDR has identified from information architecture, plain language, and transcreation.
Health equity framework: The lens this toolkit takes in health communication literacy to reach all communities including those marginalized in access to COVID-19 vaccines.
What we know: General facts and trends from residents as personas in various phases in the vaccination rollout in the US.
Tools and templates: Actionable steps and checklists to evaluate and make design and content changes to COVID-19 vaccine websites and mobile apps.
Key population considerations: Evidence-based tools and approaches to increase health equity for black and brown communities, the elderly, people with disabilities, and rural and hard-to-reach communities.
Special Topics: Insights on popular topics such as vaccine resistance and hesitancy, multilingual translation for diverse residence, and data reporting.
While collaborating with local and state governments to design vaccine webpages, we have learned that our partners are inundated with a high volume of calls and emails to their call centers. The most frequently asked questions from their residents include, but are not limited to: Where can I get vaccinated? and When am I eligible to get the COVID-19 vaccine?
“We need help with an overwhelming amount of phone calls and public health emails.”
“We receive on average 3,000 calls to our call center per day. In one week, we’ve received 30k from residents. Many questions can be answered on our website.”
As such, content managers and developers of COVID-19 digital health information tools are faced with the difficult task of imagining what your end-users will find understandable and actionable.
Although there are a number of strategies from personas to use cases to make your vaccine webpages more user-friendly, many do not account for the everyday changes in residents’ attitudes, behaviors, and wayfinding efforts related to vaccines and testing.
This toolkit aims to close the gap that exists between writers and developers and their end-users. It provides actionable steps for creating more accessible and equitable consumer-centric digital tools that have the potential to ease the burden of navigating complex digital health information.
In a short qualitative research study with a sample of six residents with varying backgrounds, demographics, and vaccination eligibility phases, we learned that, on average, residents do not know where to get vaccinated and when they will be eligible for the vaccine.
When can I get the covid vaccine?
“When am i scheduled to get the covid vaccine massachusetts”
“When do Americans get vaccines?”
“When will 1b group get vaccine”
In addition, anecdotal resident stories from our partners and web analytics confirm how residents are frustrated and are experiencing information navigation challenges. Elderly residents call first for vaccine appointment scheduling due to poor information architecture on county and state websites.
Bilingual residents receive support from their children, as translated content does not accommodate for their dialects and health literacy levels. This toolkit reduces these literacy inequities and improves the user experience of residents navigating for COVID-19 information on government digital tools.
Communication and content development teams at local and state governments vary in their COVID-19 communications response strategy to vaccinations and testing.
Answering the questions below will help you and your team understand how you can best use this toolkit:
Have you integrated health equity best practices into your COVID-19 digital communication such as on your organization's website, mobile, marketing, and social media campaigns?
There is no one easy communication solution, but we have centralized some new resources to customize your own COVID vaccination communication campaign for your community to:
communicate effectively about the COVID-19 vaccines, or vaccines in general, and
bring equity forward in your communication.
Relationships and Networks: refer to the connections and support structures made up of family (biological, adopted, or chosen), friends, romantic partners, and people within cultural communities, neighborhoods, schools, and workplaces.
Maintaining social relationships is important for maintaining health. Relationships may promote health equity with protective factors against health-harming behaviors, or intensify poorer health outcomes by enabling health-harming behaviors.
The USDR Digital Communication Toolkit reflects best practices to integrate communities and networks in content development for equitable COVID-19 vaccination distribution. The example below from the State of Pennsylvania represents a diverse population of potential website visitors, from parents to school representatives, with direct navigation to networks.
Health equity is defined as having the personal agency and fair access to resources and opportunities needed to achieve the best possible physical, emotional, and social well-being. The Health Equity Framework (HEF) centers on four spheres of influence to impact population health outcomes: 1) relationships and networks, 2) systems of power, 3) physiological pathways, and 4) individual factors.
HEF is a practical tool for communication leaders, educators, and health literacy professionals in public health research and practice. It reflects on COVID-19 digital communication tools and supports a shift toward addressing health inequities resulting from the interplay of structural, relational, individual, and physiological factors. Practical examples of the HEF are reflected in the Tools and Templates section.
Our focus is on residents’ need for accurate, timely, transparent, and equitable COVID-19 communication. HEF is reflected in the following diagram:
Systems of Power: refer to policies, processes, and practices that determine the distribution and access to resources and opportunities needed to be healthy.
Systems of power—as opposed to social conditions such as poverty—contribute to the systematic and differential treatment of groups and include institutionalized and interpersonal manifestations of bias.
Systems of power can promote health equity by ensuring fair access to resources and opportunities. Some have also been restructured to repair the historical and current causes of health disparities. The HEF views these systems as functioning at varying levels in both political (federal, state, and local) and institutional (school, private companies, health care systems) spaces.
Physiological Pathways: a person's biological, physical, cognitive, and psychological abilities.
Physiological pathways can impact health outcomes substantially. The timing and intensity of key determinants can change developmental, biological, and cognitive trajectories, leading to poorer health outcomes. For example, adults with specific learning disabilities (SLD) reported lower scores in reading comprehension, functional reading skills, and general intelligence than non-SLD groups. Individuals with SLDs identify their condition as worse in adulthood due to extended childhood adversities.
When applying physiological pathways in practice, we focus on:
Increasing awareness of how physiological responses can be driven by other spheres of influence, and
How interventions can maximize and support the resilience of physiological functions and abilities after exposure.
For any target audience, effective message development should align with the community’s values and preferences and come from trusted sources. Because COVID-19 communication needs to change over time, vaccination communication strategies must also adapt to the changing needs of residents, and evolving vaccine information, and guard against information fatigue.
Therefore, we created two personas based on current and past projects with our government partners that reflect the principles in the Health Equity Framework with strategic messaging.
Do you know someone who is unsure about taking the COVID-19 vaccine? If so, knowing their barriers and beliefs can help you understand how to start a conversation with them.
Meet Mark, an elderly citizen who is retired and a caregiver to his wife. His main frustration is the cognitive overload of vaccine information, which he reads online and sees on the news. The best messaging outreach for Mark is to position getting the COVID-19 vaccine as part of his own personal leadership role as a protector of the community.
Meet Isabella, a single mom to three children (5, 11 years old) and a housekeeper at a large health system. Although she is able to speak English on a basic literacy level, Isabella isn’t confident about getting the COVID vaccine due to its side effects. She relies on her 11-year old daughter to translate scientific terms. The best messaging outreach for Isabella is one that frames the motivation for getting vaccinated from decreasing personal risk to help others, thus preventing message reactance such as “Protect your family, if not yourself”.
We have conducted remote observations and contextual inquiry as part of a qualitative study with a small sample of residents from various phases of the COVID-19 vaccine rollout. In addition, we analyzed over 75 state and local COVID-19 vaccine websites for best practices on vaccination eligibility. This is what we learned from residents about residents' mental models:
What do you know about getting vaccines? Users' knowledge level varied about receiving the vaccine from not much, 2 doses, rolling out now, to some level of phase prioritization. People, in general, are not sure when and where to get vaccinated for Covid-19 especially for the “wait-and-see” groups.
When will you be able to get a vaccine? We also learned that timing is random based on a resident's social network, with the highest frequency mentioned in March, June, and the Fall.
How important is the vaccine in your life? Vaccine importance is role-dependent. Teachers and essential workers feel like this is very important.
How do you want to get the vaccine? There are two sides to the coin.
Realistically: Residents currently have to go somewhere, such as a hospital or community center, sign up, and wait for a response. This is slightly inconvenient for them.
Ideally: At work, so residents don’t have to travel out of their way. They want to go somewhere and to someone familiar to them, such as their Primary Care Physician.
Who should make decisions about vaccine distribution? There’s a range of responses: A mix of people, people with clout, and scientists. A December Morning Consult poll found that a majority of US adults turn to their families for vaccine guidance.
What is the role of the federal government in vaccine distribution? From residents:
“Ensure we have enough vaccines for everybody and work on distribution.”
“Make sure it’s available regardless of money and geographic area.”
“Strong federal guidelines, procedures and protocols.”
“Coordinating with state, local governments on prioritization and delivery.”
When navigating a website, users with limited literacy skills tend to:
Get distracted by extra words and elements of a website like links and icons
Navigate in a linear fashion and backtrack frequently
Choose the first answer they find, without checking if it’s correct—and have a hard time telling the difference between high- and low-quality information
Have trouble recovering from mistakes
When reading, users with limited literacy skills focus on the center of the screen. Once they shift their focus from the navigation to the center of the screen, they’re unlikely to look back to the navigation to solve a problem or change course if the content isn’t meeting their needs.
Top three search takeaways:
Search 1: Multiple searches, vague information, PDF downloads, and no answer
Search 2: State government and public health websites that highlight a prioritization framework, with no current details on next steps
Search 3: Going straight to workplace resources or to your primary care provider
Top query searches from English speakers:
"Where can I get vaccinated in my county?"
“When can I get the covid vaccine?”
“When am i scheduled to get the covid vaccine massachusetts”
“When do Americans get vaccines?”
“When will 1b group get vaccine”
Location of searches ranked from the highest influence and highest usage to lowest influence and usage:
State gov website
CDC
Health center
Public school website
Google’s common question accordion tool
BBC News
AARP, NY Times
Residents' next steps after searching for vaccine information online and offline:
Try again search in early spring
Talk to their main health provider with personal experience
Make a decision depending on the general public flow
Talk to their employer
We have identified common reading and cognitive challenges for the general public, based on existing research from trusted organizations, including health.gov. We account for the health equity principles, with a specific focus on Individual Factors and Physiological Pathways of people with disabilities, communities with low literacy skills, and people with cognitive and medical issues.
Keep the following in mind
Users with limited literacy skills generally read more slowly, and reread words, sections, or elements on a website (like buttons or menus) in order to understand them.
These users skip words or sections or start reading in the middle of a paragraph.
When users are reading something very important, and they feel the stakes are high, they try to read every word, because they can’t effectively scan and draw meaning from content.
Dense “walls of words” can trigger limited-literacy readers to skip content altogether.
For forms, users need to read the instructions and the form field labels, and then either spell the answers to questions or read and select from multiple-choice answers. This is a lot to ask from users with limited literacy skills.
This is an analysis that synthesizes a survey of seven state governments’ social media: California, Florida, Massachusetts, New Jersey, New York, North Carolina, and Oregon. Attention was put towards content that was highly interacted with. Full list of screenshots captured here.
Some governments are partnering with local organizations to create and circulate content. When content is created in partnership, it’s shared first on the partner’s account and then re-circulated by the government’s account. There’s leveraging of state and local celebrities and medical professional heroes.
There’s consistency across Twitter and Facebook and in content when it’s in more than one language. When a state organization has a COVID-related banner image and pinned content on Twitter and Facebook they are visually grabbing and simple.
A type of content that is common and highly interacted with is sharing vaccination milestones. Many times, but not always, the message was first shared by a government official’s account, such as the Governor’s, and then circulated by a department.
Governments are elevating BIPOC medical professionals to share their personal and professional voices. Amid disparities, Black doctors are using TikTok and Instagram to foster restorative justice and encourage healthy behaviors such as getting the COVID-19 vaccine.
Some governments are validating that there are vaccine worries and then addressing them. The voice is empathetic and reassuring about the feelings and decisions their residents need to make.
Acknowledging the impact of the pandemic on mental wellness is a common theme and content type and provided an option for support in social media posts.
Encouraging a staycation, a fun way to frame not traveling to support public health is another example that shows care for residents.
Messaging in physical contexts that some residents have fond memories of is powerful and encourages them to look forward to going back to.
Social media are powerful platforms that create echo chambers, especially for vaccine discourse. Each platform has its own strength and weakness but ultimately are meant to connect people and information.
Below is an analysis of the relationships black, indigenous, and people of color communities (BIPOC) have with social media, especially in terms of health information-seeking behavior.
Social media enables the broadening of marginalized communities’ social networks.
Both of similar and dissimilar communities.
A specific focus seems to be on engaging with dissimilar communities.
There is a stronger trust built with similar communities, i.e. those that have similar appearances and/or experiences.
Less education = limited access to reliable internet connectivity and technology.
Disproportionally affects Black and Hispanic communities.
Social media has dual faces:
Place for support
Discrimination
Video testimonials are effective messaging vehicles.
Particularly effective in Hispanic communities.
Themes related to public health and healthcare
General sense of distrust in large organizations.
Overarchingly low health and technology literacy percentages.
Language barriers: translators not always available and Google Translate is not good enough.
Black social media users are more likely than other BIPOC backgrounds to engage with political action via social media.
Higher percentage of belief in messages’ efficacy via social media.
Hispanic belief is similar though at a lower percentage, followed by Asian Americans.
Young BIPOC (18-49): higher likelihood of using social media than 50+.
Black & Hispanic groups believe social media helps them find like-minded communities.
8:10 BIPOC users believe social media’s efficacy in magnifying important and unnoticed issues, and representing marginalized groups.
Young BIPOC are the biggest consumers of websites created by and for people of color.
Young BIPOC individuals with less socioeconomic resources consume more online media sources than BIPOC individuals with more resources.
Sources for increasing visibility of relevant issues and support:
Black Twitter
Black Youth Project
Presente.org
LinkedIn is not a trusted social media source for Black users due to a history of BIPOC related content being removed without explanation.
Themes related to public health and healthcare
Feel as if they receive different (poorer) treatment.
Sense of distrust, feeling like guinea pigs.
Translated materials don’t resonate with audiences.
Linked below is a resource produced by (NYC Mayor’s Office for Economic Opportunity) that includes tools and tactics for civic service design regarding COVID-19 public health efforts that can also be applied to the broader design realm. Use these tips to amp up concreteness to more effectively catch your target user’s attention and make them more likely to perform the key behavior.
You can use the following audit checklist to evaluate your digital tools, such as a website, mobile app, social media content, and digital print media. This checklist centralizes recommendations derived from , ETR's , and .
What networks and relationships do people value the most to feel safe, protected, and empowered to take action on healthy behaviors? e.g. a trust messenger/ from their communities, family, friends, schools, religious institutes (church, temple, mosque).
Did you put the most important information first at the top of the page, above ?
Did you use images that facilitate learning and reduce negative emotions? e.g. avoid vaccine imagery that .
Did you make your site and documents accessible to ? Learn more about .
Did you use labels that reflect words your users know? To help different users find what they need, repeat topics under multiple categories. For example, based on card sorting, content on in our vaccine website template appears under three categories: Homepage, Find Vaccines, Phases.
We have been supporting local and state governments with evaluating their COVID-19 web and mobile pages and providing tactical recommendations for improved user experience and content literacy, education, and communication.
Our focus with these case studies is on convenience and confidence: Is it easy to get the vaccine? Is it safe to get the vaccine? We also prioritized a mobile-first experience informed by our partner's web analytics.
Below are examples of before and after we have designed for government partners with best practices in three areas:
To reduce friction on homepages or any pages above the fold to learn about COVID-19 vaccines quickly, we added:
Temporary banner to inform visitors of the most important action to take, specifically in signing up for a vaccine appointment and determining their phase eligibility
Sign-up primary call-to-action (CTA) to nudge on the primary behavior for increasing the number of mobile and web visitor sign-ups for vaccination appointments
Learn more secondary CTA to build trust and encourage visitors who have different behavioral motivations other than signing up for an appointment
To empathize with our government partner's residents, we applied role modeling strategy such as:
Images that identify with the Hispanic community's values and cultural experiences
Reusable cards to highlight vaccine information with CTA to sign up
Language preferences to automatically translate a webpage into English or Spanish for improved literacy and outreach
Color guides to differentiate high risk or valuable information to a visitor with a call to action and tactical resources that are linkable or supported with a phone number to call to.
We understand there are limited resources and time, so this was created with that in mind. This is the leanest possible way to help governments audit, strategize and deploy a social media strategy. The first session will take up to 1 hour, then we'll schedule additional workshops to dive deeper, depending on needs.
Below are multiple templates we created based on our qualitative research with bilingual residents from various states and counties with messaging that resonates. The design and content files are available for public use. To use and even edit the Figma files, you will need to create a Figma account (it's free!):
Our design and content guidelines listed below are best practices to post on social media. The guidelines are themes from generative research we conducted with residents and local and state government partners to understand vaccination messaging with BIPOC communities:
Our playbook will help you audit, strategize, and distribute trusted COVID-19 content across social media channels.
# | Guideline | Example |
1 | Images must show human faces with real skin tones and relatable activities | Relatable activities would be 4th of July BBQ, travel, and any other common activities in the primary community. Vibrant colors are good in moderation |
2 | Typography and font must align with the organization's brand guidelines to create a sense of familiarity | Examples:
|
3 | Stories matter to people. Include quotes of leaders in the community | Quotes and mini stories in FB and Instagram Images are key to grab attention on Instagram Tell people how your work and their actions are changing the lives of people. Use one person’s story to show how you’re solving the problem you’ve set out to solve. Be detailed. In some cases, it may be most compelling to include both types of information, abstract and concrete, for contrast.
|
4 | Motivate users to act and track (this is the power of social filters) and ensure frequent progress | Examples: social filters, data dashboard in social (with the right metrics) Make progress visual. See below as an example |
Coming soon.
# | Guideline | Example |
1 | To boost motivation for your desired behavior, show and add immediate benefits | “Your vaccine is waiting for you” and “reserved” versus “available” increased vaccination rates by 11% in patient SMS messaging OR partnership with local businesses like Krispy Kreme with a free donut with your vaccination card |
2 | For the benefits that are mostly functional, brainstorm some fun or emotional benefits that can be added. | “We’re excited to launch our festival X on October 10, 2021 and have your back. Your vaccine is waiting for you.” |
3 | Make benefits concrete and tangible | “Get back to what you love” “Get back to who you love” Present a way to fulfill a need for your user’s goals, NOT the county only |
4 | “We care about you and hear you. Access FREE transportation services to get you to your vaccination appointment. Get free transport here today: www.example.gov” |
5 | Youtube videos, Facebook live with tribal groups and churches, testimonials on the website, Instagram stories |
6 | Clear call to action with facts is more important than inspirational posts | Say exactly what happens with the user acts. For example, pin a post on Facebook for where to get a vaccine appointment: X example |
7 | Highlight the impact of the individual’s action(s) on the pandemic | “Your actions save lives. By wearing a mask, you protect 13k children in Pueblo who are not yet eligible for the COVID-19 vaccine” Give reminders by bundling vaccination with existing behaviors at key moments when people are already primed to think about changing their behavior. For example,
|
8 | People are more willing to perform a healthy behavior for themselves and their families/friends NOT their town. | Just asking people to do something is a way to increase an opportunity's salience. (Called the Question-Behavior Effect.) Prompts to consider our intention and likelihood of performing a behavior influence our actual behavior. Ask: 1. “Are you going to [behavior]? 2. “Will this be the year that you [behavior]?” 3. “You’ve set X health goal this year. Are you going to [behavior] this week?” “You believe in delivering high-quality care. Are you planning to [behavior]?” |
9 | Content has to be informative and insightful with direct application to COVID trends | Example of topics requested:
|
10 | People often know what they want to do or need to do, but they struggle with the how. | Social filters help to construct an implementation intention “IF I’m in situation X, THEN I will do Y action that will help me achieve my goal.” |
11 | Explain fully to people what to expect after they get tested or vaccinated Close any knowledge gap and fill their void of uncertainty. | For example, include explicit instructions as to how someone should expect after dose 2 of a Pfizer vaccine and what to expect during the end-to-end process. |
Below are examples and creative guidance to build confidence and trust with BIPOC communities, based on extensive qualitative and quantitative research from the Ad Council, including cross-cultural focus groups, to uncover the most impactful messaging frameworks.
Check out the microsite developed by Georgia Tech’s Center for Inclusive Design and Innovation with funding from CDC Foundation and technical assistance from CDC. It makes COVID-19 messaging available to people with disabilities.
For rural communities and farmers, highlight to support them to get to their vaccination appointments such as childcare and transportation
Emphasize voices of the community (trusted messengers) like promotoras/ community health workers and leaders to reach vaccine-hesitant and resistant people
Specify the when, where, and how of what you/the person will do. Example:
Information surrounding COVID-19 changes and evolves constantly, which can be overwhelming to the lay public. This picture is further complicated by the widespread misinformation and disinformation about the virus, especially on social media.
The following resources for print media, such as flyers and downloadable social media infodemics, are from trusted organizations to support your agency in public health digital outreach.
Physiological Pathways: Recognize the diversity of needs among people with disabilities and the sub-communities therein. There is no one-size-fits-all approach.
Here are some guidelines for reaching people with disabilities
Design for cognitive and visual impairment needs. Follow baseline Web Content Accessibility Guidelines and ensure ADA compliance in all online communication. Ensure screen readers and other assistive technologies are supported in the design.
Highlight accessible accommodations. Clearly highlighting accessibility accommodations at vaccine provider locations will help alleviate any fear of not being able to get to a vaccine appointment. Consider representing this accessibility (ramp access, etc) in imagery.
Relationships and Networks: Social networks can also affect the degree to which individuals accept, question, or refuse vaccination. For instance, recent research on COVID-19 vaccine hesitancy indicates that adults in Black and Latino communities are less likely to know someone or personally have received at least one dose of the vaccine, but are the most likely to want to see how the vaccine is working for other people they know.
The degree to which individuals are nudged towards vaccination uptake can be influenced again by those they are most frequently connected.
Vaccine hesitancy can be thought of as a continuum. It can range from indecision, uncertainty, delay, and then, at most severe, reluctance. Each of these forms of hesitancies can be influenced by several factors.
These are referred to as the 5 A’s: Access, Affordability, Awareness, Acceptance, Activation or the 3 C's of vaccine hesitancy: convenience, confidence, and complacency. When applying the health equity framework principles, the 5A taxonomy can help guide your vaccine campaigns’ communication and collateral strategy.
We recommend the following tactics to overcome vaccine hesitancy.
1.Moderate your organization's social media and marketing platforms by assigning a community manager to engage with residents apply the SWIFT Method to respond to vaccine misinformation:
Stop when you encounter potential misinformation. Even deciding not to share the content is a success metric.
Investigate the source. Who is sharing the information? Is this from a reputable source (sometimes there's no source, or there is imposter content)? Use Google to look up news sources.
Find better coverage. Look up what other coverage is on the same topic/ event. Focus on trusted sources by fact-checking sites. Do reverse image searches for false context of connection.
Trace claims, quotes, and media to the original context. Click through links to find the original source.
2. Provide and advertise digital testimonials from within your community networks. When authentic testimonials are not available, use personas to create a compelling and relatable story. Public figures that are closer to the community (non-governmental figures) can also be a great voice to include around acceptance.
3. Create collateral that includes the call-to-action to share the content within their networks. This can include, but is not limited to: social media # campaigns, text campaigns, free giveaways that have common-day objects that spread awareness on how (and where) to get a vaccine (e.g., refrigerator magnets). The key here is widening the number of touchpoints with positive messaging around vaccine uptake.
4. Avoid myth-busting. Don’t give misinformation a platform. Lead with the fact above the fold on your digital platforms.
5. Consider who is communicating health information in a family. In many multilingual families, there may be mono-lingual and bilingual household members. As such, tailoring vaccine messaging towards relationships can be useful. Messaging could come directly from those most impacted by a person’s place on the vaccine hesitancy continuum and transition them to vaccine acceptance.
For example, consider Isabella. In her case, health information was tailored to emphasize the benefit of getting vaccinated to protect her family members (children, parents who might live with her) may be an effective way to motivate healthy behavior.
Individual Factors: Acknowledge individual beliefs and attitudes towards the COVID-19 vaccine access in messaging. This is a great time to acknowledge misinformation about who has access to COVID-19 vaccines and local availability.
6. Highlight convenience and experience-based information about vaccine services. Appeal to beliefs that might delay vaccination due to perception of inconvenient provider locations or time spent.
7. Identify key concerns constituents in your area have about affordability. Clarify those questions up-front in content.
8. Clearly state the role services play in vaccine cost. State whether insurance status will affect their situation, and whether reimbursement is required.
Individual Factors: Writing multilingual content requires messaging that aligns with the intent and values of your residents' language and dialects. Simply using Google Translate doesn't resolve dialect and values transported in a language.
Transcreation is creative translation. It is the act of changing a text to make its meaning culturally responsive to your audience. By transcreating content, you are not simply transferring verbatim text from one language to another. Rather, you are considering slight nuances and cultural subtleties that could cause the meaning to be lost in the process of translation.
By allowing creative agency in the translating process, a professional transcreator can ensure that content across many languages retains its true intent, tone, and style while allowing for variations in the copy to ensure understandability, resonance, and health communication/health literacy best practices are still in place.
An example: The word “drug” is often used to describe medication in health communication in US English. However if you were to translate directly to Spanish the word would be “drogas” which would not be typically associated with medications in a Spanish-speaking community. So although using the term “medicamento” or “medicinas” may seem to raise the level of necessary reading comprehension, this term will be better understood and more accessible to the community you are trying to reach. This is the transcreation mindset.
Here are some recommendations
Test content with both a mix of bilingual and monolingual speakers to ensure that the new transcreated version satisfies the intent of the messaging.
Create content that also captures the diversity of the United States and be creative with translation strategies - recognizing colloquial adaptations in the language (hybrid bilingual conversational languages e.g., Taglish, Spanglish, etc).
Always check the level of reading competence in both languages to ensure that content understandability is maintained through the transcreation process. Best practice for English and other language content is at most 5th-grade reading level and below.
Provide a creative brief. If using localization services to transcreate content, provide not just the source copy but also a creative brief (for instance, the key considerations in this Toolkit could be a great place to start).
Create your content strategy with multiple languages in mind at the same time. This prevents English-based copy from being drafted in silos and failing to resonate with large bilingual communities across America. Drafting both versions simultaneously can help save time and money.
Tip: Transcreation also goes beyond words and into the look, feel, style, and imagery used within digital communication mediums. See the Key Population Considerations section for tips on how to incorporate a Health Equity Framework in developing your communication style and design.
We recommend the following Covid-19 resources for non-English speakers.
We recommend the following Covid-19 resources for Spanish speakers.
In December 2020, we created a vaccine website template, designed for communication and development teams to launch their own vaccine website or webpages in hours. Below are links to step-by-step instructions and a design for content managers, designers, and developers to use for their county and states.
We applied all of the communication best practices, which we listed in the checklist, in our designs.
The template is designed to meet the needs of the majority of counties. It’s built on WordPress, which is an easy platform to set up and customize for your own county with limited technical knowledge. It is simple to maintain and update during vaccine distribution. In addition, this user guide is written for public health officials – not tech experts - who are familiar with Internet basics.
USDR's vaccination website template free to government providers and community-based organizations.
A step-by-step guide to launch the template on WordPress within days.
Below is a mobile-view design template with applied health literacy and design thinking best practices that your organization can use.
Individual factors: concern a person’s attitudes, skills, and behaviors, which are shaped by their personal experiences, including their relationships with others and access to opportunities, often driven by systems of power.
Social determinants of health, such as poverty, unequal access to health care, lack of education, stigma, and racism shape individual factors and contribute to health inequities. Healthy childhood development of social and emotional skills is associated with better mental and physical health outcomes, life satisfaction, and life expectancy in adulthood.
Below is an example from the State of Hawaii that successfully demonstrates content on mental health support on one of their vaccine webpages.
To organized content with information scent, we:
Prioritized most important information in top button such as Vaccine sign-up instead of Data Dashboard
Provided secondary links to important pages (testing, reopening)
Separated resources or links to other authorities (e.g. CDC) to prevent overwhelming users with content
Set a clear hierarchy of user goals by setting apart vaccine scheduling even more with clear steps to guide their decision-making process
Reorganize content to give users information, rather than direct them to it (i.e. with a “Q&A” format)
Minimize scrolling by redesigning key design elements, so users can get information quickly
Relationships and Networks: Community-based organizations from parent groups to national coalitions are championing their own communities to engage parents and youth around the COVID-19 vaccine. Therefore, parents and peer-to-peer networks play an important role in protecting our communities from COVID-19.
Below are resources to support parents in communities to get their kids vaccinated and empower youth and adolescents to be trusted messengers to their peers.
Systems of Power: noncitizen immigrants face a range of potential access-related barriers to obtaining a COVID-19 vaccination.
According to KFF, noncitizen immigrants are more likely than citizens to be uninsured and, as a result, are less likely to have a usual source of care as well as more likely to delay or go without it and to have concerns about its costs.
People who are uninsured may be more likely to have concerns about the potential costs associated with obtaining the vaccine.
Below are resources to support undocumented workers and their employers with flyers, occupation letters, and undocumented immigrant letters provided by NYC Epicenter.
We have listed outreach channels to reach marginalized populations, hard-to-reach, rural communities, and other identities such as undocumented workers, those with limited digital literacy levels, and uninsured people.
The list is based on literature and landscape review and ongoing discussions with state and local government partners and community-based organizations. It includes push/ outbound and pull/ inbound marketing methods to meet people where they are at.
TV ads. The Colorado Department of Health and Environment has released commercials in English and Spanish featuring Colorado health care workers who are people of color, promoting the message that vaccines are safe.
Radio ads to reach undocumented workers, the uninsured, farmers, and digital desserts
Spotify and Pandora Ads
Social media toolkits such as HHS' We Can Do This Kit
Edutainment (entertainment-education) like comic books and cartoonish flyers to reach young kids and adolescents. Extensive research has shown efficacy in leveraging telenovela/fotonovela style communication in Latino communities. Another example is the work the KINA (TOGETHER), a series of projects headed by the University of Minnesota designing and developing in partnership with area Native American communities to create programs that share the exciting world of science with children in Kindergarten to 6th grade.
Reminder/recall approaches (postcard, letter, telephone, or combination)
Sound trucks to spread awareness of mobile COVID-19 vaccine clinics such as in Quebec
SMS and phone banking such as VaxDirect, which pulls tactics from phone banking from elections
Reserved appointments each week for high-risk neighborhoods where vaccinations have lagged, releasing them on a different day and only to residents of those areas
Appointments allocated for the weekend with access to transportation and other social services like food and tied to other benefits such as WIC and SNAP benefits
Door-to-door knocks with mobile device partnerships such as mPulse with leaders from the community. North Carolina has partnered with faith leaders to ensure communities of color and underserved communities have access to vaccinations at the state’s mass vaccination clinics, including releasing appointments to Black and Latinx church attendees before opening up registration to the general public.
Family member and child vaccine appointment scheduling with child immunization schedule cards in vaccine patient portals
Community-based partnerships like fraternities and sororities, HBCUs, and public libraries. Tennessee has an African American Health Care Clinician Workgroup, with working members from the NAACP, the Black Nursing Society, and other Black organizations, who are disseminating messaging on the importance of vaccinations and will ultimately help vaccinate Black communities. West Virginia is funding faith-based community members and people of color to administer COVID-19 vaccines directly to communities of color, ascribing to the principle that having trusted, local figures helping with distribution will improve those communities’ confidence in the vaccine
Vaccinations offered at major social and sporting events such as the Milwaukee Bucks offering Pfizer COVID-19 vaccines to eligible fans 16+ who are attending the game against the Nets on Sunday (on ABC) at Fiserv Forum
Virtual town halls to dispel COVID-19 vaccine myths and resources
Training Trusted messengers, promotoras, and community health workers with process improvements to their workflows
Local business partnerships like Krispy Creme in drive-thrus
Airport for testing and vaccination spots to reach tourists and travelers
Dollar tree as located clinics to reach low-income households within dollar store distances
Vaccine equity clinics and mobile vaccination vans to reach rural, farmers, and hard-to-reach communities
The Centers for Disease Control and Prevention (CDC) created the Crisis and Emergency Risk Communication (CERC) to share lessons learned during past public health emergencies and research in the fields of public health, psychology, and emergency risk communication.
The CERC program provides training, tools, and resources to help health communicators, emergency responders, and leaders of organizations communicate effectively during emergencies.
Systems of Power: The obstacles faced by residents and healthcare providers in rural areas are vastly different than those in urban areas. There are many factors that create healthcare inequities and impede rural residents from achieving the highest care and health. These include economic conditions, access, cultural and social differences, educational shortcomings, lack of recognition by legislators, and the sheer isolation of living in remote areas.
Here are some guidelines for communicating with rural and hard-to-reach communities
Recognize transportation barriers and offer a solution. Especially in rural environments, transportation inconvenience or lack of access will be top-of-mind. Offer solutions/options in your communication plan to help provide better information about physical access to COVID-19 vaccines.
Offer mailed information to communities where internet bandwidth may be limited or not consistent. Low internet bandwidth is a reality in many rural communities. Try different outreach methods, leveraging digital communications in a printed format to reach this constituency. This can be automated by using bulk messaging actions through healthcare provider EHRs.
Answer questions on financial concerns. Clarify the free-offering of vaccines and that there are no hidden costs by healthcare providers.
Offer resolution regarding religious considerations. Religious communities are often a foundation in rural communities and provide access to health information, a sense of community belonging, and social events. Use digital media to provide examples of trusted community members receiving the vaccine, while also keeping a sense of fatalism (fatalismo) that’s a cornerstone in many religions and even secular communities.
Agency/freedom of choice is paramount in rural communities.
Address strong attitudes in rural areas regarding the risk of disease transmission. There has been research that residents of rural areas have less worry about coronavirus transmission compared to urban areas. Nearly half of rural residents surveyed felt that the seriousness of the coronavirus is “generally exaggerated” .. To reach this audience, it is important to highlight the benefits of vaccination that may emphasize values that go beyond community immunity and/or risk of severe disease. Meet your constituents with what they value most.
Utilize social media for reach, but invest in maintaining comments. Although in rural areas, public health departments are often overleveraged and understaffed, there are remote options for hiring Community Managers that are digital natives and trained in support/help content response to monitoring your Facebook Pages, Twitter, Youtube comments, etc. This can be a rich source of engagement and scaling, as they can field oncoming comments that would otherwise be turned off because of internal department resource constraints.
Dispell misinformation and reframe the narrative. Avoid the urge to “mythbust” - in a 10-second skim, it’s just as easy for a reader to not see the word “Myth” as it is for them to read the statement you’re trying to debunk.
Relationships and Networks: Those living with family and/or caregivers are more likely to engage in vaccinations than those who are living alone (based on studies of influenza vaccinations). Specify by age-range.
Here are some guidelines for reaching the elderly and aging populations
Tailor COVID-19 messaging to address different living situations of the aging populations in your communities. They will have different motivators.
Message directly to the caregivers of the elderly to motivate, educate, and create awareness around COVID vaccinations.
Specify who is your primary audience. Not all elderly identify as “older adult and/or at risk”.
Recognize the tendency to be biased toward seniors we know. Be careful of individual bias in your content strategy - content writing to cater to one’s own grandparent, rather than writing for the population you’re targeting and the diversity therein.
Individual Factors: A person’s attitudes, skills, and behaviors are shaped by their personal experiences, including their relationships with others and access to opportunities. In aging populations, these factors can be influenced not only by age, but also by their cultural constructs of health and wellness, educational level, independence, agency over their health decisions, and more.
Address those who have not utilized medical services in the past 3 months. Medical service use is another influencing factor of vaccine uptake. Target your messaging to those less likely to have already received prior notices on vaccine availability. If they have not received medical services recently, they also have not received medically-vetted information about vaccine availability from a medical professional they trust or know.
Recognize perceived barriers and offer a solution. Some individuals, particularly those who are still independent, may have perceived transportation inconvenience (lack of access) or financial concerns. Acknowledge perceived barriers and highlight solutions in your messaging (e.g., clarity on the cost of the vaccine and clarify that there are no hidden costs by healthcare providers; help them locate facilities near public transportation options).
Highlight expected differences in transient COVID vaccine side effects in comparison to vaccines they are more familiar with. Many individuals in this age range are familiar with the Shingles vaccine, which is communicated to potentially disrupt up to 3 days of daily behavior.
Do not assume tech illiteracy. Tech literacy is growing amongst the 50+ community, thus closing the mobile divide more than ever. According to the AARP, smartphone adoption is up to 81% for those 60 to 69 surveyed (n= 849/2607 ), and 62% of those 70+ (n= 776/2607 ).
Do not assume they are digital natives. Although digitally engaged, it’s still important to consider that this population is not a digital native. So, it’s important to create a User Interface flow to address questions and route to online booking (maybe not their first preference) versus calling into hotlines/call centers (perhaps their first assumed step).
Physiological Factors: With age comes many health challenges, both chronic and acute. As such, many aging community members are relying on healthcare services and/or care networks (family or institutional) to address their day-to-day needs. For vaccine communication, it’s key to address any interrelationships between age, medications, and immunological factors that are considerations for vaccine uptake OR contribute to potential vaccine hesitancy.
Consider visual impairment needs. Use large fonts and ample spacing between lines of text in both digital and print assets. If print materials are being provided, use matte paper stock (high gloss causes a glare) and high contrast between text and background.
Amplify utility of written content to cater to those with hearing loss. The benefits of reducing call-volume are twofold: workforce scalability and better patient experiences for those who may require assistance due to hearing-loss. By emphasizing motivation to share more print/digital content to reach those with hearing impairment, you also reach many others. This concept is called the curb-cut effect. Half of US adults 60+ have hearing loss.
Local and state government agencies and community-based organizations have the opportunity to impact COVID-19 vaccination rates in the US to eliminate vaccine-preventable COVID-19 infections. This work is prevention at its purest level, and its impact will be felt for generations to come. The USDR Covid Digital Communications Toolkit supports your communication teams with content and messaging tools with the following goals:
Increase COVID-19 vaccination rates in the United States across all 50 states.
Eliminate racial disparity and reduce geographic disparities in COVID-19 vaccination.
The following logic model is a high-level overview of the flow of materials and processes for equitable communication during COVID-19 vaccine distribution.
Systems of Power: Place-based health metrics like these capture key contributors to the risk of getting COVID-19 or having a worse outcome including poverty, reliance on public transportation, and crowded housing.
The National Academies’ report recommends place-based measures of social vulnerability, such as the Centers for Disease Control & Prevention Social Vulnerability Index (SVI) or the COVID-19 Community Vulnerability Index (CCVI), which includes racial, ethnic, and language composition of a census tract.
News around COVID-19 vaccines is evolving quickly. As we learn more, we will add new and relevant information to this toolkit. You can subscribe for future updates.
If you would like more information or pro-bono support from our teams of technologists at USDR, please reach out. We will get back to you within hours.
If you found this toolkit helpful, please share it with other vaccination communication content developers and educators who might benefit from this information.
A. P., V. C., & D. Y. (2020, August 19). The Health Equity Framework: A Science- and Justice-Based Model for Public Health Researchers and Practitioners - Amy Peterson, Vignetta Charles, David Yeung, Karin Coyle, 2020. Retrieved February 14, 2021, from https://journals.sagepub.com/doi/full/10.1177/1524839920950730
ETR. (2020, August 19). ETR's Health Equity Framework. Retrieved February 14, 2021, from https://www.etr.org/about-us/health-equity-framework/
Holt-Lunstad, J., Smith, T. B., & Layton, J. B. (2010, July 27). Social Relationships and Mortality Risk: A Meta-analytic Review. Retrieved February 16, 2021, from https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1000316
Nguyen, S. (2020, December 31). 3-Day Research Sprint: How residents look for Covid-19 vaccine information [Policy Memo]. Los Angeles: US Digital Response. Retrieved February 14, 2021, from https://bit.ly/3tYdmzT
Patton, G. C., Olsson, C. A., Skirbekk, V., Saffery, R., Wlodek, M. E., Azzopardi, P. S., . . . Sawyer, S. M. (2018, February 22). Adolescence and the next generation. Retrieved February 16, 2021, from https://www.nature.com/articles/nature25759
Patterson, M. B., & Mellard, D. (2008, May). Contrasting Adult Literacy Learners With and Without Specific Learning Disabilities. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3229155/
Peterson, A., Charles, V., Yeung, D., & Coyle, K. (2020). The Health Equity Framework: A Science- and Justice-Based Model for Public Health Researchers and Practitioners. Health Promotion Practice, 152483992095073. doi:10.1177/1524839920950730
State of Pennsylvania. COVID Vaccines. Retrieved from https://www.health.pa.gov/topics/disease/coronavirus/Vaccine/Pages/Vaccine.aspx
State of Hawaii. (2021, February 13). COVID-19 Vaccine. Retrieved from https://hawaiicovid19.com/vaccine/
Ardila, A., Bertolucci, P. H., Braga, L. W., Castro-Caldas, A., Judd, T., Kosmidis, M. H., . . . Rosselli, M. (2010, December 01). Illiteracy: The Neuropsychology of Cognition Without Reading. Retrieved from https://academic.oup.com/acn/article/25/8/689/4384
Colter, A., & Summers, K. (2014). Eye Tracking with Unique Populations: Low Literacy Users. In J. Romano Bergstrom & A. J. Schall (Eds.), Eye Tracking in User Experience Design (pp. 331–346). Waltham, MA: Morgan Kaufmann Publishers/Elsevier
Nguyen, S. (2020, December 31). 3-Day Research Sprint: How residents look for Covid-19 vaccine information [Policy Memo]. Los Angeles: US Digital Response. Retrieved February 14, 2021, from https://bit.ly/3tYdmzT
ODPHP. (2016, June 8). What We Know About Users with Limited Literacy Skills. Retrieved from https://health.gov/healthliteracyonline/what-we-know/section-1-1/
Amee. (2017, November 24). What is the Fold? The Crazy Egg Glossary. Retrieved from https://www.crazyegg.com/blog/glossary/what-is-the-fold/
ETR. (2020, August 19). ETR's Health Equity Framework. Retrieved February 14, 2021, from https://www.etr.org/about-us/health-equity-framework/
Secretary, H. O., & Office of the Chief Information Officer (OCIO). (2021, January 21). Accessibility Compliance Checklists. Retrieved from https://www.hhs.gov/web/section-508/accessibility-checklists/index.html
SF.gov. (2021, January). Get notified when it's your turn for the vaccine: San Francisco. Retrieved from https://sf.gov/get-notified-when-its-your-turn-vaccine/form
ODPHP. (2016, June 8). What We Know About Users with Limited Literacy Skills. Retrieved from https://health.gov/healthliteracyonline/what-we-know/section-1-1/
Raskin, A., & Zahorian, I. (2021, February 10). When can I get vaccinated?: Resource Analysis (February 2021). Retrieved from https://docs.google.com/presentation/d/1_jAbQxtWglbvrxDWgvOapE_2PtHenM-LjwhQQmjcfLQ/present#slide=id.gbb0d6d51e7_0_174
Rosenwald, M. (2020, December 26). 'A needle makes my blood run cold': Will the phobic get the coronavirus vaccine? Retrieved from https://www.washingtonpost.com/local/needles-fear-coronavirus-vaccine/2020/12/22/1c554500-408a-11eb-8db8-395dedaaa036_story.html
ADC Council. (2021, February). Messaging that Resonates. Retrieved from https://adcouncilvaccinetoolkit.org/messaging
National Center for Immunization and Respiratory Diseases. (2018, January 25). Shingles Vaccination. Vaccines and Preventable Diseases. https://www.cdc.gov/vaccines/vpd/shingles/public/shingrix/index.html
NCAPPS. (2021, January). Health Care Person-Centered Profile. Retrieved from https://ncapps.acl.gov/covid-19-resources.html
Nelson Kakulla, B. (2020, January). 2020 Tech Trends of the 50+. AARP Research. https://www.aarp.org/research/topics/technology/info-2019/2020-technology-trends-older-americans.html
Reed, N. S., Ferrante, L. E., & Oh, E. S. (2020). Addressing Hearing Loss to Improve Communication During the COVID-19 Pandemic. Journal of the American Geriatrics Society, 68(9), 1924–1926. https://doi.org/https://doi.org/10.1111/jgs.16674
International Council on Active Aging. (2011). ICAA’s Guidelines for effective communication with older adults. http://www.changingthewayweage.com/Media-and-Marketers-support/guidelines.htm
Wooten, K. G., Wortley, P. M., Singleton, J. A., & Euler, G. L. (2012). Perceptions matter: Beliefs about influenza vaccine and vaccination behavior among elderly white, black and Hispanic Americans. Vaccine, 30(48), 6927–6934. https://doi.org/10.1016/j.vaccine.2012.08.036
Berkeley Media Studies Group. (2020, December 8). Communicating about the COVID-19 vaccines: Guidance and sample messages for public health practitioners. Berkeley Media Studies Group. http://www.bmsg.org/resources/publications/communicating-covid-19-vaccines-guidance-and-sample-messages-for-public-health-practitioners/
Despres, C. (2021, February 17). Bilingual Comic Strip Helps Latinos See Benefits of COVID-19 Vaccine. Salud America. https://salud-america.org/bilingual-comic-strips-covid-19-vaccines/
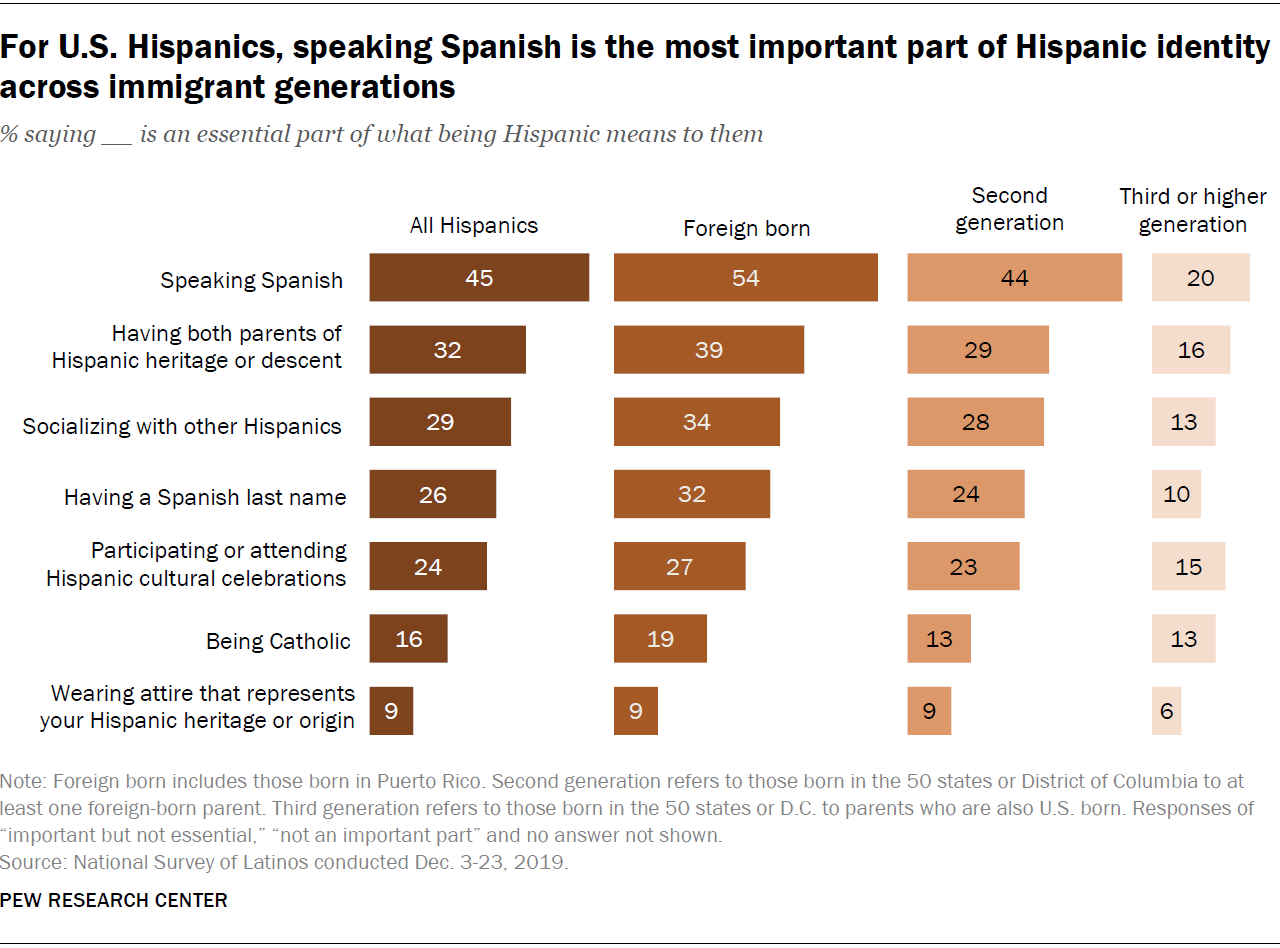
For U.S. Hispanics, speaking Spanish is the most important part of Hispanic identity across immigrant generations. (2020, September 23). Pew Research Center. https://www.pewresearch.org/wp-content/uploads/2020/09/FT_20.09.21_HispanicIdentity_3b.png
Gonzalez-Barrera, A. (2020, September 24). The ways Hispanics describe their identity vary across immigrant generations. Pew Research Center. https://www.pewresearch.org/fact-tank/2020/09/24/the-ways-hispanics-describe-their-identity-vary-across-immigrant-generations/
Hamel, L., Kirzinger, A., Lopes, L., Kearney, A., Sparks, G., & Brodie, M. (2021, January 27). KFF COVID-19 Vaccine Monitor: January 2021 - Vaccine Hesitancy. Kaiser Family Foundation. https://www.kff.org/report-section/kff-covid-19-vaccine-monitor-january-2021-vaccine-hesitancy/
Hudnut-Beumler, J., Po’e, E., & Barkin, S. (2016). The Use of Social Media for Health Promotion in Hispanic Populations: A Scoping Systematic Review. JMIR Public Health and Surveillance, 2(2), e32. https://doi.org/10.2196/publichealth.5579
Hugo Lopez, M., Gonzalez-Barrera, A., & López, G. (2017, December 20). Latino Identity Declines Across Generations as Immigrant Ties Weaken. Pew Research Center’s Hispanic Trends Project. https://www.pewresearch.org/hispanic/2017/12/20/hispanic-identity-fades-across-generations-as-immigrant-connections-fall-away/
Kearney, A., Lopes, L., & Brodie, M. (2021, January 14). Vaccine Hesitancy Among Hispanic Adults. Kaiser Family Foundation. https://www.kff.org/coronavirus-covid-19/poll-finding/vaccine-hesitancy-among-hispanic-adults/
McKenna, M. (2020, November 11). Winning Trust for a Vaccine Means Confronting Medical Racism. Wired. https://www.wired.com/story/winning-trust-for-a-vaccine-means-confronting-medical-racism/
Menasce Horowitz, J., Brown, A., & Cox, K. (2019, April 9). The role of race and ethnicity in Americans’ lives. Pew Research Center’s Social & Demographic Trends Project. https://www.pewresearch.org/social-trends/2019/04/09/the-role-of-race-and-ethnicity-in-americans-personal-lives/
Moran, M. B., Chatterjee, J. S., Frank, L. B., Murphy, S. T., Zhao, N., Chen, N., & Ball-Rokeach, S. (2017). Individual, Cultural and Structural Predictors of Vaccine Safety Confidence and Influenza Vaccination Among Hispanic Female Subgroups. Journal of Immigrant and Minority Health, 19(4), 790–800. https://doi.org/10.1007/s10903-016-0428-9
Muvuka, B., Combs, R. M., Ayangeakaa, S. D., Ali, N. M., Wendel, M. L., & Jackson, T. (2020). Health Literacy in African-American Communities: Barriers and Strategies. HLRP: Health Literacy Research and Practice, 4(3), e138–e143. https://doi.org/10.3928/24748307-20200617-01
Nielson. (2021). Latinx Community. Diverse Intelligence Series. https://www.nielsen.com/us/en/about-us/community/latinx
Schmid, P., Rauber, D., Betsch, C., Lidolt, G., & Denker, M.-L. (2017). Barriers of Influenza Vaccination Intention and Behavior – A Systematic Review of Influenza Vaccine Hesitancy, 2005 – 2016. PLOS ONE, 12(1), e0170550. https://doi.org/10.1371/journal.pone.0170550
The National Museum of African American History and Culture. (n.d.). I Am A Person Committed To Equity. Talking About Race. Retrieved February 18, 2021, from https://nmaahc.si.edu/learn/talking-about-race/audiences/committed-equity
The Permanente Medical Group. (n.d.). Protecting Yourself and Your Family during COVID 19. Retrieved February 15, 2021, from https://mydoctor.kaiserpermanente.org/ncal/video/protecting-yourself-and-your-family-from-covid-19-1722442
The Permanente Medical Group. (n.d.). Staying Safe from COVID-19. My Doctor Online. Retrieved February 18, 2021, from https://mydoctor.kaiserpermanente.org/ncal/video/staying-safe-from-covid-19-1701986
Vaccine Central | National Resource Center for Refugees, Immigrants, and Migrants (NRC-RIM). (n.d.). Retrieved February 18, 2021, from https://nrcrim.umn.edu/vaccines/vaccine-central
Centers for Disease Control. (2021, January 20). Rural Communities. COVID-19. https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/other-at-risk-populations/rural-communities.html
Kirzinger, A., Muñana, C., & Brodie, M. (2021, January 7). Vaccine Hesitancy in Rural America. Kaiser Family Foundation. https://www.kff.org/coronavirus-covid-19/poll-finding/vaccine-hesitancy-in-rural-america/
CDC. (2018, January 23). Crisis & Emergency Risk Communication (CERC)|CDC. Retrieved from https://emergency.cdc.gov/cerc/index.asp
MacDonald, N. E., & SAGE Working Group on Vaccine Hesitancy. (2015). Vaccine hesitancy: Definition, scope and determinants. Vaccine, 33(34), 4161–4164. https://doi.org/10.1016/j.vaccine.2015.04.036
Rosselli, R., Martini, M., & Bragazzi, N. L. (2016). The old and the new: vaccine hesitancy in the era of the Web 2.0. Challenges and opportunities. Journal of Preventive Medicine and Hygiene, 57(1), E47-50.
SAGE Working Group. (2014). Report of the SAGE Working Group on Vaccine Hesitancy. World Health Organization. https://www.who.int/immunization/sage/meetings/2014/october/SAGE_working_group_revised_report_vaccine_hesitancy.pdf?ua=1
Piltch-Loeb, R., & DiClemente, R. (2020). The Vaccine Uptake Continuum: Applying Social Science Theory to Shift Vaccine Hesitancy. Vaccines, 8(1), 76. https://doi.org/10.3390/vaccines8010076 Thomson, A., Robinson, K., & Vallée-Tourangeaub, G. (2016). The 5As: A practical taxonomy for the determinants of vaccine uptake. Vaccine, 34(8), 1018–1024. https://doi.org/10.1016/j.vaccine.2015.11.065
Centers for Disease Control and Prevention. (2016). Everyday Words for Public Health Communication. https://www.cdc.gov/other/pdf/EverydayWordsForPublicHealthCommunication.pdf
Health Literacy Tool Shed. (2021, February). https://healthliteracy.bu.edu/
Agency for Healthcare Research and Quality. (2019, November). Short Assessment of Health Literacy–Spanish and English (SAHL-S&E). Health Literacy Measurement Tools (Revised). https://www.ahrq.gov/health-literacy/research/tools/index.html#short
AMA. (2021, January). The role of data collection in the COVID-19 pandemic. Retrieved from https://www.ama-assn.org/delivering-care/health-equity/role-data-collection-covid-19-pandemic
Bernard, S., & Zylla, E. (2020, November 6). Advances in States’ Reporting of COVID-19 Health Equity Data. Retrieved from https://www.shvs.org/advances-in-states-reporting-of-covid-19-health-equity-data/
Relationships and Networks: Within many communities, there are different dynamics to social networks and how information is transmitted and trusted. Each community is diverse and the key is identifying key influencers or influencing relationships in the community that will amplify your digital communication strategy.
Identify key influencer(s) and represent them in your content or as part of your dissemination and outreach campaigns. This is especially important considering recent research that shows that adults in Black and Latino communities are less likely to know someone, or personally have received at least one dose of the vaccine, yet also most likely to want to see how the vaccine is working for other people they know. Getting more testimonials out there digitally with far reach will increase relationship-based transmission of health behaviors. Leverage the scale of digital media to reach beyond someone’s local network with a resonant testimonial.
Here are some guidelines for reaching Black and Brown communities
Racism is a risk factor for COVID, not race. If discussing race and COVID vaccinations, be clear on your intent. You need to be specific as to how the two relate (racism and systemic inequalities and vaccine availability/uptake/trust) and what action items your message is trying to convey.
Don’t assume a shared identity in your content outreach strategy. There are many communities within the Black and Brown Communities. It’s important to not assume that there is one identity shared across these communities. About 50% of Hispanic adults say they most often describe themselves by their family’s country of origin or heritage, using terms such as Mexican, Cuban, Puerto Rican, or Salvadoran.. (Gonzalez-Barrera, 2020) About three-quarters of Black adults say that being Black is extremely (52%) or very (22%) important to how they think about themselves; by comparison, about six-in-ten Hispanic (59%) and 56% of Asian adults say being Hispanic or Asian is extremely or very important to their identity.
Avoid assumptions of homogeneity in linguistic preferences. There is significant linguistic diversity in America’s Black and Brown communities, so your communication strategy needs to take this into account and not center your outreach strategy on language alone. Speaking Spanish is seen as a key part of Hispanic identity; use this to consider how to reach this population. For U.S. Hispanics, Speaking Spanish Is the Most Important Part of Hispanic Identity across Immigrant Generations.
Acknowledge valid concerns regarding vaccine safety. Given the historical context of medical misconduct towards Black and Brown communities, there are generational impacts to the trust that the medical community has not earned back. Recognizing this history of inequities and social justice issues, and the lower rates of clinical trial participation from these racial groups, address concerns with humility while also reassuring them of Covid-19 vaccine safety and efficacy.
Present clear information on side effects versus safety issues. Highlight the differences between expected brief reactions to the vaccine versus critical safety issues. For example, of those who have been vaccinated, 45% had minor side effects, 7% moderate, and none severe.
Recognize barriers and offer a solution. Some individuals, particularly those who are still independent, may have perceived transportation inconvenience (lack of access) or financial concerns. Acknowledge perceived barriers and highlight solutions in your messaging (e.g., clarity on the cost of the vaccine and clarify there are no hidden costs by healthcare providers; help them locate facilities near public transportation options).
Consider trust and agency in healthcare communication with these communities. We need to earn trust and recognize the imperative to give people the agency over their own selves and the self-efficacy to provide for their own wellbeing. The decision is ultimately theirs. These values should be reflected in word choices and imagery in all health communication outreach. Trust in state governments may defer by age group. In recent research, younger Latino adults are less trusting than older Latinos of government as a source of information about the COVID-19 vaccine. Their confidence was highest from their own healthcare provider.
Leverage imagery that resonates and is diverse. Stock images are often quite saturated and are entrenched in institutional biases. Consider looking locally to hire photographers in the community you’re trying to reach and put forward images that inspire and connect with your constituency. This includes diverse images of people and scenery, which is localized and represents your communities' surroundings best (urban v. rural, local communities and diversity, local fashion choices, etc).
Consider modalities that resonate within certain communities. Extant research has shown efficacy in leveraging telenovela/fotonovela style communication in Latino communities. See below for an example.
Use media outlets that resonate within communities. 11% of surveyed Latinos in a recent study by Nielson reported social media as their trusted source of information on coronavirus as compared to 10% for government websites.
Ask community culture brokers to help spread the word and serve as a mediator. Build relationships with trusted messengers from diverse organizations and community groups. Find individuals in the local community that has been vaccinated to build trust and to widen the net of those who know someone who has had successful experiences with vaccination (use of video, written, media testimonials).
Work closely with the IHS on outreach communication to the Tribal Nations.
Identify local channels for community health (e.g., Promotoras) and ask for their participation in a video testimonial, news segment, social media campaign, etc.
Leverage local religious institutions to reinforce vaccine availability information and services. Again, ask for their participation in local campaigns and content design.
Recognize concerns on immigration status/documentation. Acknowledgment of one’s concern for safety is key to also sharing messages of vaccine availability and access. Offer . If possible, assure them that healthcare providers are not legally obligated to report nor document immigration status at the point of care.
Leverage seamless bilingual content strategy. Many individuals use multiple languages interchangeably or have specific language preferences depending on the modality (written versus spoken). Others speak only English but culturally identify with linguistic norms within their own communities. In communications, it’s important to think creatively beyond word-for-word translations to reach these dynamic language audiences. (See section).
We thank many people who contributed to this toolkit, including:
Elham Ali, MPH, PMP
Hidemi Nagao Peck, MA, MPH
Maria Flores, PhD
Jan Overgoor, PhD
Diego De Rutte
Jay Stakelon
Madeleine Lee
Jennifer Strickland
Megan O'Rorke
Joy Prescott
Our government partners




























































{kind=link}